
A Sponsor Playbook For Matching AI Use Cases To Readiness, Risk, And ROI
By Karen Maduschke, principal, ClinTech Strategy Partners

For a growing share of pharma R&D organizations, AI is quickly becoming part of the operating model. Hence, the question is no longer whether to start. It is where to go next: Which AI investments are likely to deliver measurable returns, and how should sponsors implement them without creating new regulatory, operational, or change management risk?
For many sponsors, the first AI use case has been the safest one: document workflow automation. TMF completeness checks, regulatory submission drafting, clinical study report generation, and internal document summarization are sensible starting points. They’re high volume, repetitive, and comparatively easier to govern when human review, version control, and established documentation workflows remain intact. In fact, the Tufts CSDD/DIA 2025 global assessment found that around 38% of companies have implemented AI for TMF management and 32% for clinical study report writing.1 If your organization hasn't started yet, this remains the right entry point for the same reasons; what follows applies once you're past that first deployment.
The harder question is what comes next. Enrollment-related AI, including feasibility, site selection, and patient recruitment, promises some of the largest measurable returns. Data quality and monitoring sits on a regulatory tailwind from ICH E6(R3). Document workflow can continue to scale but may no longer be the highest-value frontier. None is universally right. The right next step depends less on which use case sounds most exciting than on whether the problem you're solving matches your organization's regulatory exposure, data readiness, process maturity, change capacity, and honest build-versus-buy position.
This article offers a practical sequencing framework for deciding whether the next AI investment should deepen document automation, move into data quality and monitoring, or pursue enrollment-related AI across feasibility, site selection, and patient recruitment.
Start With The Problem, Not The Technology
It probably goes without saying for most R&D leaders: AI is a means not an end. But the pressure to deploy AI can quietly invert that logic. The right starting point is a well-defined operational pain that AI is genuinely positioned to solve, not a capability looking for a problem.
Three pain points dominate the conversation, and all three have credible AI applications:
Enrollment failure. Nearly 80% of clinical trials miss their enrollment timelines.2 A 2024 Tufts CSDD analysis revised the long-cited cost-of-delay figure: A single day of delay now represents roughly $500,000 to $800,000 in lost prescription revenue, substantially lower than the $8 million figure that circulated for 30 years, but still significant when multiplied across portfolios.3
Protocol complexity and data over-collection. Phase 3 protocols now average 5.96 million data points, with a 283% increase in data points and a 40% increase in procedures over the past decade. Roughly one-third of procedures do not directly support primary, key secondary, or safety endpoints.4 ICH E6(R3), effective in the EU since July 2025 and adopted as final FDA guidance in September 2025, directly addresses this through its emphasis on risk-based, fit-for-purpose data collection.5,6
A related upstream use case is AI-supported protocol optimization: assessing protocol complexity, eligibility criteria, visit schedules, patient and site burden, and avoidable data collection before the study is launched. For many sponsors, this should not be treated as a separate AI program. It is a decision-support layer that can improve feasibility planning, sharpen recruitment assumptions, and strengthen risk-based quality management before operational problems are locked into the protocol.
Documentation burden. TMF management, CSR drafting, and submission-ready data set generation continue to consume disproportionate clinical operations capacity. This is the use case most sponsors have already tackled but few have scaled beyond initial pilots.
What's The Realistic Upside?
The honest answer is less than vendor pitches suggest, more than skeptics fear, and highly dependent on baseline maturity.
The most defensible public benchmarks come from the Tufts CSDD/DIA 2025 assessment, which surveyed 302 respondents from 79 sponsor and CRO organizations. Across 36 distinct clinical development activities, teams reported an average 18% cycle time reduction from AI-enabled work.1 The single highest-impact use case was identifying targeted patient communities, with reported time savings of 68%.1 AI applied to risk and quality assessment showed 40% adoption among surveyed organizations; identifying diverse patient populations reached 52%.1
Vendor-published case studies routinely report higher numbers: 70%+ reductions in TMF processing time, dramatic acceleration of CSR drafting, and double-digit improvements in screen failure rates. These claims may well be accurate in the specific deployments described, but they're rarely independently verified, rarely include the full implementation and validation cost, and rarely report the cases where the deployment underperformed expectations.
A more useful position is to treat peer-reviewed and consortium data as a defensible floor and vendor claims as the optimistic ceiling while designing every pilot to measure actual ROI in your environment. The KPIs that matter — cycle time delta, query volume reduction, screen failure rate, validation effort, ongoing operational cost, site burden, and adoption — should be defined before contract signature, baselined against current state, and tracked through the pilot. If your pilot doesn't produce defensible internal numbers, you have a demonstration rather than a learning. The only ROI figure that matters for your next funding decision is the one your own organization can stand behind.
A Readiness Diagnostic
Before committing to a next-step investment, run a brief diagnostic against the conditions that determine whether AI will deliver returns. The point is not to produce a perfect maturity score. It is to expose the gap between the use case you want and the operating conditions required to make it work.
Five factors determine readiness for the next AI investment: regulatory proximity, validation burden, data foundations, process standardization, and change capacity. The table below maps each factor across lower- and higher-readiness signals, with the implication for use case selection. It is designed to be used by clinical operations, quality, regulatory, digital, and procurement leaders together before the build-versus-buy discussion begins.
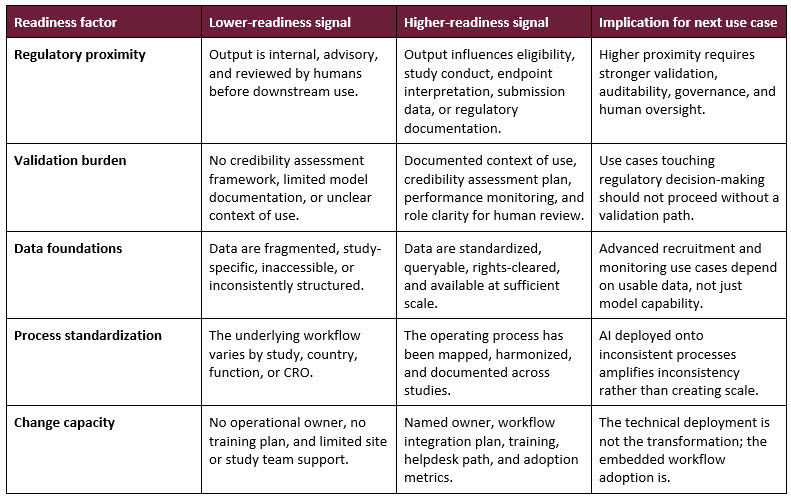
A simple example makes the sequencing logic concrete. A sponsor with mature eTMF processes but fragmented EHR access should probably not jump directly to recruitment AI, even if recruitment has the highest theoretical ROI. It may get faster returns by scaling TMF completeness checks and applying AI-enabled anomaly detection to standardized EDC data while building the data access foundation, site workflow, and privacy model that recruitment AI will require later.

Mapping Readiness To Use Case
Lower regulatory proximity, lower data maturity: Extend document workflows. If your organization is still maturing on data infrastructure and process standardization, the safer next move is to deepen the document workflow use case rather than jump to a higher-stakes one. Scale TMF automation from pilot to portfolio. Extend CSR drafting support or regulatory-document review to additional therapeutic areas. Build internal validation and change management muscle on use cases that do not directly determine patient eligibility, dosing, endpoint adjudication, or submitted clinical data.
Moderate regulatory proximity, moderate-to-strong data maturity: Invest in data quality and monitoring. Centralized statistical monitoring, anomaly detection, and risk-based quality management (RBQM) sit in a sweet spot for many organizations: meaningful ROI, a clear regulatory tailwind from ICH E6(R3), and a more manageable validation curve relative to recruitment AI. The output supports human decision-making rather than replacing it, which keeps the credibility bar proportionate to the context of use.
Higher regulatory proximity, strong data maturity: Pursue enrollment-related AI. The returns are potentially the largest, but so is the readiness bar. Enrollment-related AI is not a single capability. Feasibility AI predicts country- and indication-level enrollment potential before site outreach. Site selection AI ranks investigator sites against historical performance and capacity data. Patient recruitment AI operates at the patient identification layer, typically through NLP-based screening of EHR or registry data. The three share data prerequisites but represent distinct operational integrations, and most sponsors will sequence them rather than deploy them simultaneously.
Across all three, prerequisites include historical enrollment performance, site activation timelines, investigator site capacity data, EHR access agreements, privacy controls, site engagement, patient contact pathways, and the operational integration to convert AI-flagged candidates into enrolled patients. Without them, enrollment-related AI generates predictions and lists, not study participants.
A note for EU-operating sponsors: the EU AI Act's timeline should be built into sequencing decisions. The act becomes broadly applicable from August 2026, but obligations for high-risk systems are subject to category-specific transition timelines, including later dates for certain high-risk areas and for systems embedded into regulated products.7 AI tools that influence eligibility, recruitment selection, or clinical decision-making should be classified case by case with regulatory, quality, legal, and privacy input rather than assumed to fall into a single timeline.
Build, Buy, Or Hybrid?
This is a question that gets less airtime than it deserves: Not every AI use case requires a vendor relationship. Sponsors routinely default to "buy from our existing platform vendor" or "ask our CRO to add the capability," when the best path for some use cases may be internal deployment using enterprise large language model (LLM) licenses and the right operational governance.
The decision turns on three factors: data sensitivity, validation burden, and depth of specialist capability required.
Candidates for internal deployment. Use cases that operate on internal documents, don't touch submission data, and benefit from organizational context tend to lend themselves to in-house AI built on enterprise LLM platforms. Examples include internal protocol consistency checking, summarization of internal meeting notes and operational documents, draft generation for internal communications, and first-pass review of internal SOPs against updated guidance. The infrastructure exists, the regulatory exposure is low, and the validation burden is internal.
Candidates for vendor or CRO partnership. Use cases that require validated GxP-compliant infrastructure, cross-study data access at scale, integration with EDC, CTMS, eTMF, or safety systems, or deep specialist AI capability, such as, for example, clinical-text NLP at scale, privacy-preserving access to institutional data, validated signal detection, or software classified as SaMD are not realistic in-house builds for most sponsors. The validation, integration, and ongoing maintenance costs can eclipse the platform cost.
Hybrid models. A growing pattern is sponsors deploying internal AI for upstream work such as draft generation, internal summarization, or first-pass review, then contracting with vendors for downstream validated workflows. The internal layer creates leverage; the vendor layer carries the regulatory weight.
The cost difference between paths is often an order of magnitude or more. The risk is that sponsors conflate the categories: contracting for a vendor solution to do internal document summarization or attempting to build in-house for a use case that genuinely requires validated infrastructure. Match the deployment model to the use case, not to your incumbent vendor's road map.
A Note On The Broader R&D Life Cycle
The lens of this article is clinical operations: patient recruitment, data quality and monitoring, and document workflow. But sponsors face AI investment decisions across the full drug development life cycle. The same diagnostic can be adapted to other parts of the drug development life cycle, but the specific readiness signals will differ.
Pharmacovigilance is a useful comparison point because AI deployment is relatively mature for high-volume, predictable tasks such as Individual Case Safety Report intake and processing, literature surveillance, and signal triage. The CIOMS Working Group XIV report on AI in pharmacovigilance, published in December 2025, provides an internationally-aligned governance reference for PV applications.8 The lesson for clinical operations is not that PV should displace near-term trial execution priorities. It is that sponsors generate more durable returns when use cases are selected against the maturity of the data, the clarity of the process, the regulatory expectations, and the ability to keep humans appropriately in the loop.
The five-factor diagnostic still applies; what changes is how each factor is interpreted for the life cycle stage and the specific context of use.
From AI Playbook To Operating Discipline
AI ROI in clinical R&D does not come from choosing the most ambitious use case. It comes from matching the use case to the organization's regulatory exposure, data readiness, process maturity, and honest assessment of whether the capability should be built internally or contracted for.
Two patterns predictably stall AI investments:
Pilot without portfolio intent. A pilot that isn't designed to scale is a demonstration, not an investment. Define the path from single-study pilot to multi-study deployment before contracting, including the validation, training, and integration work that scaling requires.
Under-resourced change management. The technical deployment is rarely where AI investments fail. The failure point is operational integration: clear ownership, embedded workflows, and the training capacity to maintain adoption after the launch enthusiasm fades.
The sponsors generating durable returns are the ones treating AI deployment as an operational program with the same rigor applied to any other clinical operations transformation: defined problem, defined owner, defined success measure, defined validation path, and a realistic view of what their organization can absorb.
The next AI investment that pays back is the one that solves a problem you can articulate, with data you can access, in a process you can change.
References:
- Lamberti MJ, Florez MI, Do H, et al. "The Adoption and Use of Artificial Intelligence and Machine Learning in Clinical Development." Therapeutic Innovation & Regulatory Science. 2025;59(5):1074-1086. https://pubmed.ncbi.nlm.nih.gov/40439837/
- "Streamlining Clinical Trials: Mitigation and Management." Applied Clinical Trials. December 2025. https://www.appliedclinicaltrialsonline.com/view/streamlining-clinical-trials-mitigation-and-management
- Smith ZP, DiMasi JA, Getz KA. "New Estimates on the Cost of a Delay Day in Drug Development." Therapeutic Innovation & Regulatory Science. 2024;58(5):855-862. https://pubmed.ncbi.nlm.nih.gov/38773058/
- TransCelerate BioPharma and Tufts CSDD. "Insights Informing Strategies for Optimizing the Collection of Clinical Trial Data." Therapeutic Innovation & Regulatory Science, 2026. https://www.transceleratebiopharmainc.com/initiatives/optimizing-data-collection/
- European Medicines Agency. ICH E6 Good Clinical Practice — Scientific Guideline, effective July 23, 2025. https://www.ema.europa.eu/en/ich-e6-good-clinical-practice-scientific-guideline
- U.S. Food and Drug Administration. E6(R3) Good Clinical Practice (GCP), final guidance, September 2025. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/e6r3-good-clinical-practice-gcp
- European Commission. EU AI Act, high-risk provisions applicable from August 2026. https://digital-strategy.ec.europa.eu/en/policies/regulatory-framework-ai
- Council for International Organizations of Medical Sciences (CIOMS). Artificial Intelligence in Pharmacovigilance — Working Group XIV Report. Geneva: CIOMS; published 4 December 2025. https://cioms.ch/working_groups/working-group-xiv-artificial-intelligence-in-pharmacovigilance/
About The Author:
 Karen Maduschke spent two decades leading clinical trial technology globally, most recently as senior director and general manager at IQVIA, where she held P&L responsibility for the company's global eConsent business serving 60+ pharma sponsors and investigator sites in nearly 100 countries. She now advises senior R&D and health technology leaders on technology-enabled transformation, operating model readiness, and the realities of deploying AI in regulated clinical environ
Karen Maduschke spent two decades leading clinical trial technology globally, most recently as senior director and general manager at IQVIA, where she held P&L responsibility for the company's global eConsent business serving 60+ pharma sponsors and investigator sites in nearly 100 countries. She now advises senior R&D and health technology leaders on technology-enabled transformation, operating model readiness, and the realities of deploying AI in regulated clinical environ