
From CRO Management To Networked Governance: The New Quality Imperative
By Partha Anbil, MIT Sloan life sciences industry advisor, and Jayanthi Anbil, consultant

Outsourced clinical development remains a structural feature of biopharma, but the operating model that once emphasized transactional vendor management now requires broader governance built for decentralized execution, digital data flows, and heightened scrutiny of sponsor accountability.1,2,3,4 Quality breakdowns in outsourced trials should be understood as symptoms of weak system design across governance, vendor oversight, data flows, and escalation pathways.1,2,3,5 The practical implication for life sciences leaders is that modern outsourcing cannot be controlled through contracts and periodic audits alone; it must be managed through a connected, risk-based quality architecture spanning sponsors, CROs, specialist vendors, trial sites, and digital platforms.1,2,4,5
The outsourced clinical trial environment is now far more complex than the classic sponsor-CRO model. Sponsors may simultaneously rely on laboratories, eConsent and eCOA providers, telehealth workflows, wearable device vendors, home health services, centralized monitoring partners, and cloud-based data environments, all of which can influence participant safety and data reliability.1,2,3,4 In such an ecosystem, failures often emerge at interfaces as unclear accountability, weak change control, poor data lineage, inadequate system validation, delayed escalation, or insufficient alignment between critical-to-quality factors and oversight intensity.2,3,4,6
Current Regulatory Environment
The FDA’s final guidance on conducting clinical trials with decentralized elements makes clear that greater operational flexibility does not dilute sponsor or investigator responsibility.1 Sponsors are expected to decide which trial activities are appropriate for remote execution, ensure personnel are properly trained, preserve participant safety, and maintain the reliability of trial data when work is distributed across settings and vendors.1 This is especially important in hybrid or decentralized studies, where operational convenience can unintentionally create new control gaps if remote processes are added without corresponding oversight mechanisms.1,5
ICH E6(R3), finalized in January 2025, reinforces this direction by shifting GCP further toward quality by design, fit-for-purpose controls, and active risk management throughout the trial life cycle.2 Rather than treating quality as retrospective verification, the guideline emphasizes prospectively identifying factors critical to participant protection and data credibility, then building proportionate controls around them.2,5 For outsourced studies, that means sponsor oversight must be intentional, documented, and responsive to actual risk.2,6
The 2023 EMA guideline on computerized systems and electronic data in clinical trials adds a major digital governance dimension to outsourced trial quality.3 It clarifies expectations around validation, security, access control, traceability, data governance, and supplier oversight for systems that create, transform, or store regulated clinical data.3 As more trials depend on interconnected applications and cloud-hosted environments, sponsors need to treat computerized systems as quality-critical infrastructure rather than back-office tools.3,7
What Has Changed Operationally?
Vendor management is now ecosystem management. Sponsors work through layered outsourcing structures in which primary CROs may subcontract work to specialty vendors, while key quality signals may originate outside the sponsor’s direct operational view.1,3,6 That structure can improve flexibility and access to expertise but also increases the chance that no single party sees the whole risk picture in time to intervene effectively.5,6
A second change is the growing maturity of risk-based quality management (RBQM). Recent evidence suggests that adoption has increased, but it remains uneven across organizations, with barriers including limited organizational knowledge, inconsistent change management, and mixed perceptions of value.8 RBQM is evolving as a management model that links protocol design, centralized analytics, issue detection, escalation, and remediation across the study life cycle.2,5,8 Organizations that implement it superficially may generate dashboards without meaningfully improving control over the most consequential risks.5,8
A third shift is the increased importance of exception management. Routine governance may appear effective when studies are stable, but real weaknesses often surface during protocol amendments, vendor transitions, technology outages, staffing turnover, or local execution problems.1,3,6 In those moments, quality depends on whether decision rights are clear, escalation paths are tested, residual risk is reassessed, and corrective actions are tracked to effectiveness rather than closure alone.2,5,6

Priorities For Quality Leaders
Quality leaders should start by defining an explicit sponsor accountability architecture. Decision rights, delegated activities, escalation triggers, and oversight responsibilities need to be visible across governance charters, quality agreements, monitoring plans, data review plans, and vendor management processes.1,2,6 When those accountabilities are fragmented across disconnected documents, recurring issues tend to remain open too long because operational ownership is diffuse.6
A second priority is vendor criticality segmentation. Not all providers should be managed with the same intensity; oversight should be calibrated to impact participant safety, endpoint reliability, informed consent, source data generation, investigational product handling, or core data processing.2,5,6 A flat oversight model can waste effort on low-risk suppliers while under-controlling the vendors most likely to create inspection findings or data credibility concerns.5,6,9
Third, sponsors should strengthen digital supplier governance. Computerized systems that support consent, endpoint capture, safety reporting, randomization, remote visits, or data integration require structured validation, change management, issue tracking, access governance, and documented oversight proportional to their role in trial conduct.3,7 Procurement onboarding alone is not enough for these providers because configuration changes, software updates, integration failures, or incomplete audit trails can create compliance and data integrity risk even when site execution appears sound.3,7
Fourth, organizations should move from static KPIs to decision-useful quality signals. Useful signals help leaders detect emerging problems before inspection, database lock delay, or participant-impacting events force reaction.5,8 Examples include recurring deviations by process step, CAPA recurrence, lagging training after protocol amendments, issue aging by vendor, system downtime affecting endpoint capture, unexplained consent anomalies, and unresolved excursions against quality tolerance limits.1,2,3,5
Operating Model For 2026
A practical operating model for outsourced clinical trial quality should integrate five disciplines into one management system.2,3,5
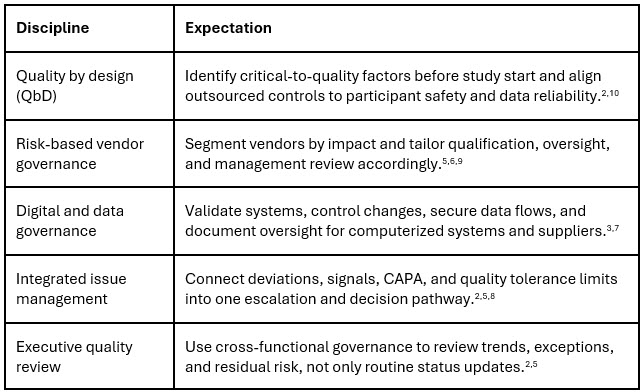
This model is more demanding than earlier outsourcing playbooks, but it is also more realistic for the current environment.2,5 Modern outsourcing succeeds when quality is engineered into the trial operating system rather than inspected into the record at the end.5,10
Strategic Implications
For sponsors, quality capability is now a competitive asset in outsourced development. Organizations that can integrate protocol design, vendor strategy, digital oversight, and risk-responsive governance are better positioned to scale global studies, adopt decentralized methods responsibly, and defend trial reliability under inspection.1,2,3 Those that treat quality as a downstream audit function remain vulnerable to systemic failures that are operationally predictable but organizationally unowned.5,6
For CROs and vendors, the environment increasingly rewards transparency, validated processes, and demonstrable control over subcontractors and digital systems.3,6,7 Strategic partners are expected to share meaningful leading indicators, manage exceptions visibly, and operate within sponsor-defined quality objectives rather than rely on retrospective performance summaries alone.5,6
For quality assurance leaders, the role is expanding from auditor to architect of the clinical quality operating model. The function now needs to connect governance, analytics, technology assurance, and vendor oversight while preserving the independence required to challenge weak assumptions before they become inspection findings or patient-impacting failures.2,3,5 The central quality challenge in outsourced clinical trials is not whether activities are externalized, but whether the sponsor has built a governance system capable of controlling a distributed clinical network in real time.1,2,3
References:
- U.S. Food and Drug Administration. Conducting Clinical Trials with Decentralized Elements: Guidance for Industry, Investigators, and Other Interested Parties. 2024. Available at: https://www.fda.gov/media/167696/download
- International Council for Harmonisation. ICH E6(R3) Guideline for Good Clinical Practice. Step 4 Final Guideline; 2025. Available at: https://database.ich.org/sites/default/files/ICH_E6%28R3%29_Step4_FinalGuideline_2025
_0106.pdf - European Medicines Agency. Guideline on Computerized Systems and Electronic Data in Clinical Trials. 2023. Available at: https://www.ema.europa.eu/en/documents/regulatory-procedural-guideline/guideline-computerised-systems-and-electronic-data-clinical-trials_en.pdf
- eClinical Forum. Requirements for Electronic Data for Regulated Clinical Research. 2024. Available at: https://eclinicalforum.org/DesktopModules/EasyDNNNews/DocumentDownload.ashx?portalid=0&moduleid=454&articleid=281&documentid=200
- European Commission Expert Group. Risk Proportionate Approaches in Clinical Trials. Available at: https://health.ec.europa.eu/system/files/2017-08/2017_04_25_risk_proportionate_approaches_in_ct_0.pdf
- Veeva. Study Oversight Implications of ICH GCP E6(R3) for Fully Outsourced Sponsors and Studies. 2025. Available at: https://www.veeva.com/eu/resources/ich-gcp-e6r3-implications-on-fully-outsourced-sponsors-and-studies/
- Florence Healthcare. A Comprehensive Guide to the EMA’s Guidelines on Computerized Systems and Electronic Data Management in Clinical Trials. 2023. Available at: https://www.florencehc.com/blog-post/a-comprehensive-guide-to-the-emas-guidelines-on-computerized-systems-and-electronic-data-management-in-clinical-trials/
- Hurley C, et al. Comprehensive Assessment of Risk-Based Quality Management (RBQM) Across the Clinical Trial Industry. Ther Innova Ragul Sci. 2024. Available at: https://pubmed.ncbi.nlm.nih.gov/38366107/
- Brookwood Global. Focus on the Things That Matter: A Risk-Proportionate Approach to Clinical Trial Management. Available at: https://www.brookwood-global.com/Focus-on-the-things-that-matter-a-risk-proportionate-approach-to-clinical-trial-management
- Duke-Margolis Institute for Health Policy. Integrating Quality by Design (QbD) and Risk-Based Approaches in Clinical Trials. 2024. Available at: https://healthpolicy.duke.edu/sites/default/files/2024-02/Slide%20Deck_Building%20Quality%20into%20the%20Design%20and%20Conduct%20of%
20Clinical%20Trials.pdf
Disclaimer: The views expressed in the article are those of the authors and not of the organizations they represent.
About The Authors:
 Partha Anbil is at the intersection of the life sciences industry and management consulting. He is currently an industry advisor, life sciences, at MIT, his alma mater. He held senior leadership roles at WNS, IBM, Booz & Company, Symphony, IQVIA, KPMG Consulting, and PWC. Anbil has consulted with and counseled health and life sciences clients on structuring solutions to address strategic, operational, and organizational challenges. He was a member of the IBM Industry Academy, a highly selective group of professionals inducted by invitation only, the highest honor at IBM. He is a healthcare expert member of the World Economic Forum (WEF).
Partha Anbil is at the intersection of the life sciences industry and management consulting. He is currently an industry advisor, life sciences, at MIT, his alma mater. He held senior leadership roles at WNS, IBM, Booz & Company, Symphony, IQVIA, KPMG Consulting, and PWC. Anbil has consulted with and counseled health and life sciences clients on structuring solutions to address strategic, operational, and organizational challenges. He was a member of the IBM Industry Academy, a highly selective group of professionals inducted by invitation only, the highest honor at IBM. He is a healthcare expert member of the World Economic Forum (WEF).
 Jayanthi Anbil has over 15 years of experience in the life sciences industry. Until recently, Jayanthi served as a global business intelligence manager at ICON Plc. She has demonstrated both quantitative and qualitative skills through primary and secondary market research. Her experience includes client services, supporting portfolio sales executives, and program/project management through commitment, start-up, checkpoint, and closure with excellent communication, people skills, and team orientation.
Jayanthi Anbil has over 15 years of experience in the life sciences industry. Until recently, Jayanthi served as a global business intelligence manager at ICON Plc. She has demonstrated both quantitative and qualitative skills through primary and secondary market research. Her experience includes client services, supporting portfolio sales executives, and program/project management through commitment, start-up, checkpoint, and closure with excellent communication, people skills, and team orientation.