
How Clinical Research Site Operating Models Perform in Practice – Part 2
By Kurt Mussina, CEO, Paradigm Clinical Research, and co-founder, Association of Multisite Research Corporations (AMRC)

Not all research sites are created the same, as we learned in part one of this series wherein, we established a taxonomy for making sense of today’s clinical research site landscape. Now, part two turns that framework into a practical operating-model analysis, asking not simply what type of site a business claims to be, but how that model performs when speed, patient access, investigator engagement, quality, accountability, and scalability are put under pressure. From freestanding research clinics and embedded private-practice sites to site networks, hospital-based models, and pure-play approaches, the article examines where each structure creates strategic advantage and where it can introduce risk. The central question is one sponsors increasingly need to answer: Which models are built not just for reach, but for controlled, repeatable trial performance?
How Clinical Research Site Operating Models Perform In Practice
The sections that follow look more closely at how site operating models perform in practice ― where each creates advantage, where each creates risk, and why model fit matters for commercial outpatient trials.
This discussion covers:
- Freestanding research clinics: strong operating control, speed, consistency, and research-native workflows.
- Embedded private-practice research sites: strong patient access, physician trust, and specialty relevance.
- Investigator models: the operational implications of employee PIs, contracted private-practice PIs, and mixed structures.
- Site networks and SMO-style models: breadth and reach, but often with less direct control.
- Hospital and academic medical center models: essential for certain trials but often mismatched for commercial outpatient studies.
- Pure-play models: clear narratives, but concentrated model risk.
- Governed hybrid models: an alternative approach designed to combine access and control under one disciplined operating system.
The Strengths Of Freestanding Research Clinics
Freestanding research clinics are the operational backbone of many high-performing commercial site businesses. They are purpose-built for trial execution, not ordinary medical offices conducting studies as a secondary activity. They are designed around protocol visits, sponsor communication, regulatory documentation, participant scheduling, recruitment workflows, monitoring access, investigational product handling, EDC entry, and query resolution.
Freestanding research clinics typically provide dedicated research staff, research-specific SOPs, centralized operational management, direct performance management, consistent participant experience, and clearer sponsor/CRO communication. For CROs and sponsors, the value is execution certainty. For investors and boards, the value is operating leverage and control.
These clinics are particularly well suited for many commercial outpatient studies, including vaccine, infectious disease, endocrinology, obesity, pulmonology, dermatology, rheumatology, device, diagnostic, and high-volume outpatient protocols. The main strength is not merely the physical clinic. The strength is that the clinic is research-native ― the clinic is designed around trial performance.
Because freestanding clinics are built around research workflows rather than adapted around them, they can also create a fundamental advantage in study start-up speed. Contracting, regulatory review, staffing, scheduling, participant flow, and activation processes can be standardized and executed with fewer institutional dependencies.
Why speed matters
Study start-up remains a major industry pain point. WCG’s 2024 study start-up materials report that, for Phase 1-3 trials over the prior three years, median trial activation was 8.12 months for AMCs and hospitals compared with 4.37 months for independent sites and physician practices.2
That finding should not be overgeneralized. Some academic and hospital sites are excellent. Some independent sites are poor. But the directional point is strategically important: Institutional environments often carry structural activation burdens that independent and physician-practice site environments may avoid.
Slow start-up is not merely inconvenient; it affects enrollment timelines, revenue conversion, sponsor confidence, site selection behavior, and the ability to recover from delayed activation across a portfolio. Freestanding commercial sites are structurally advantaged when they use standard budget positions, centralized regulatory workflows, dedicated activation teams, defined internal turnaround times, and parallel rather than purely sequential start-up processes.
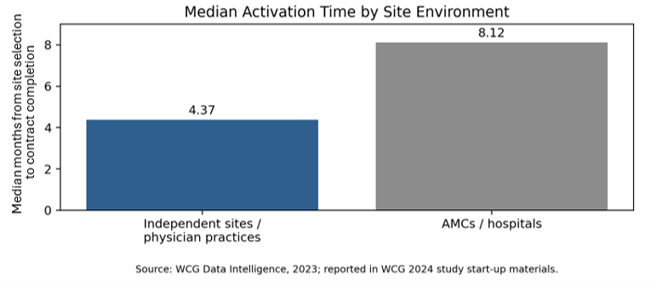
Figure 1. WCG-reported median activation time by site environment. The data supports the argument that institutional environments often face materially longer start-up timelines than independent and physician-practice settings. Source: WCG Data Intelligence, 2023; reported in WCG 2024 study start-up materials.2

The Strengths Of Embedded Private-Practice Research Sites
Embedded private-practice research sites solve a different problem: patient access through treating physician relationships. Many commercially relevant trial populations are already managed inside community physician practices. Patients with diabetes, obesity, asthma, COPD, dermatologic disease, rheumatologic disease, cardiovascular risk, chronic infections, and other outpatient conditions are often seen in private-practice settings long before they appear in a hospital research department.
A well-structured embedded model allows research to operate close to the point of care. Embedded private-practice research operations can provide access to established patient panels, specialty-specific patient identification, chart-level prescreening, warm referral pathways, community-based trial access, and better fit for chronic outpatient conditions.
This model is especially powerful when the physician practice is not expected to become a research company on its own. The practice should provide clinical credibility, patient relationships, disease-state expertise, and investigator engagement. The research company should provide staff, SOPs, regulatory support, technology, recruitment workflows, sponsor/CRO communication, training, quality oversight, and performance management. That operating logic becomes even more important when local private-practice physicians serve as contracted PIs rather than employees of the site platform.
The Investigator Model: Employee PIs, Contracted Private-Practice PIs, and Mixed Structures
Operating model is not defined only by facility type, ownership structure, brand architecture, integration status, or growth path. It is also defined by investigator model. Whether a research site company employs PIs, contracts with local private-practice physicians, or uses a mixed structure materially affects patient access, medical oversight, control, responsiveness, and scalability.
An employee PI model can increase control. Employed PIs may be more available for study conduct, easier to schedule, more directly trained, and more aligned with the organization’s operating cadence. The tradeoff is that an employee PI is unlikely to provide the same access to an active private-practice patient panel unless the physician also maintains meaningful clinical practice relationships.
A contracted private-practice PI model solves a different problem. Local physicians bring patient panels, longitudinal care relationships, specialty credibility, and patient trust. That can be a major recruitment and retention advantage. NCI/HINTS data indicate that healthcare providers are highly trusted sources of clinical trial information and can play an important role in trial awareness and participation.3
The risk is that contracted PIs can become bottlenecks if the research site company does not provide adequate operating support or if physician involvement is treated as a passive affiliation.
The stronger model, defined in this paper as the governed hybrid model, is more specific: contracted private-practice PIs supported by employee sub-Is, centralized infrastructure, common SOPs, quality oversight, recruitment support, and sponsor/CRO communication standards.
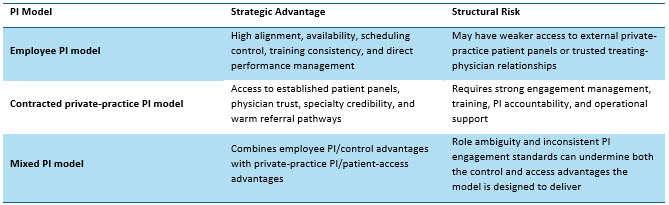
Table 4. Investigator model is a cross-cutting operating-model dimension. The strongest structure often balances direct operating control with contracted private-practice physician access.
This distinction also helps separate a governed hybrid platform from a site network. Contracting with local physicians as PIs is not the same as operating a network of independent sites. In a governed hybrid model, the physician contributes medical leadership, patient access, and clinical credibility while the research site company controls the operating infrastructure. Control does not require employing every physician. Control requires owning and governing the research operating infrastructure.
The Site Network/SMO-Style Model: Breadth Without Control
A site network, including businesses historically referred to as site management organizations (SMOs), typically consists of independently owned sites, physician practices, or local research businesses that receive services from a central organization. Those services may include business development, feasibility support, contracting and budget support, regulatory assistance, recruitment support, technology, and training.
The model has real advantages. It can create broad nominal reach, offer sponsors and CROs a single access point to many sites, and expand geographic or therapeutic-area coverage without the capital and time required to open or acquire every location. For some protocols, network affiliates may be useful as supplemental access channels.
Service provision is not operating control
If the underlying sites are independently owned and locally managed, the network may be able to advise, support, train, and measure, but it may not control the variables that determine execution: staffing levels, coordinator performance, investigator prioritization, recruitment urgency, documentation quality, or corrective-action enforcement.
This is why site count can overstate capability. A network with a large number of affiliated sites may have less executable capacity than a smaller site company with fewer but fully controlled, consistently managed locations. AMRC’s positioning work reinforces the importance of looking past nominal site count by noting that a minority of high-performing sites contributes disproportionately to trial enrollment while a meaningful portion of sites contributes little.1
Pure-play and mixed-play network risk
As a pure play, the network model can scale quickly on paper, but nominal reach can grow faster than operating control. The result may be variable execution, accountability ambiguity, weaker enrollment forecasting, thinner quality enforcement, and enterprise-value vulnerability if affiliate relationships are non-exclusive or portable.
As part of a mixed platform, network affiliates can also dilute an otherwise controlled operating story. A company may own and tightly manage some sites while merely representing, supporting, or coordinating others. That creates two materially different classes of sites under one brand promise. For sponsors, CROs, investors, and boards, the distinction should be explicit: network affiliates can be useful access channels, but they should not be presented as controlled operating assets.
Why Hospital-Heavy Models Are Often Mismatched For Commercial Outpatient Trials
Hospitals, academic medical centers, and health systems are essential to clinical research. They are often the right environment for inpatient studies, ICU studies, oncology studies, surgical studies, advanced imaging studies, rare disease studies concentrated at tertiary centers, complex specialty trials, studies requiring institutional infrastructure, and trials involving procedures unavailable in community settings.
The issue is not capability. The issue is fit.
For many commercial outpatient trials, hospital-heavy models introduce structural disadvantages, including slower contracting, coverage analysis delays, pharmacy and ancillary department dependencies, competing care-delivery priorities, less flexible scheduling, complex participant navigation, and longer institutional approval chains.
The WCG start-up data discussed in Section 3 supports this directly: median activation at AMCs and hospitals ran nearly twice that of independent sites and physician practices across the same study period.2 Hospitals can be indispensable for the right trials, but for commercially executable outpatient studies, hospital infrastructure may become a burden rather than an advantage.
Hospital-based execution can also impose higher participant burden: parking complexity, campus navigation, longer visits, less flexible scheduling, and greater institutional distance from ordinary care settings. For many outpatient studies, a freestanding clinic or embedded private-practice site may offer a better participant experience.
The Strengths And Limitations Of Pure-Play Models
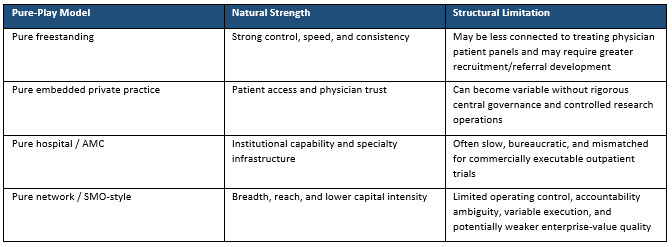
Each pure-play model discussed has a natural strength and a corresponding structural weakness. The strategic question is not which model is easiest to describe. The question is which model creates the best combination of access, control, speed, quality, accountability, and scalability.
A Look Ahead: The Promise Of The Governed Hybrid Model
In part three, the discussion moves from comparing operating models to explaining why a governed hybrid platform may offer the strongest balance of patient access, physician trust, operational control, speed, and scalability. The article will examine what makes the governed hybrid model strategically superior, why central governance is essential to avoid hybrid chaos, and how sponsors, CROs, site operators, and other stakeholders can evaluate whether a site’s operational model is truly controlled, repeatable, and built for consistent execution.
References:
- Association of Multisite Research Corporations (AMRC). “AMRC Positioning Paper.” January 2025. https://amrc.org/wp-content/uploads/2025/01/AMRC-Positioning-Paper.pdf
- WCG. “Decoding the Top Site Challenges of 2024: Study Start-Up.” 2024. https://www.wcgclinical.com/wp-content/uploads/2024/12/Decoding-the-Top-Site-Challenges-of-2024-Study-Start-Up-Slides.pdf
- National Cancer Institute. “Clinical Trial Participation Among US Adults.” HINTS Brief 48. https://hints.cancer.gov/docs/Briefs/HINTS_Brief_48.pdf
About The Author:

Kurt Mussina is CEO of Paradigm Clinical Research. With nearly 40 years of experience across clinical research, CRO, CDMO, and biopharmaceutical industries, Kurt has built and scaled organizations, driven profitable growth, and fostered long-term relationships with sponsors, CROs, and the broader clinical research community.
Prior to Paradigm, Kurt spent nearly a decade with Fresenius Medical Care (FMC), where he built Frenova, FMC’s clinical research site business, and served as the company’s President. He previously served as President of Triangle Research Labs and Senior Vice President of Aptiv Solutions, which was acquired by ICON. His experience also includes executive roles spanning global commercial operations, research and development, and business development at some of the world’s leading contract research services providers.
Kurt began his career as a chemist with Teva Pharmaceuticals and Novartis. He later earned his MBA from Duke University and moved into leadership roles focused on biopharma operations and strategic partnerships.