
Why Operating Model Is The Next Competitive Frontier In Clinical Research Site Strategy – Part One
By Kurt Mussina, president, Paradigm Clinical Research, and co-founder, Association of Multisite Research Corporations (AMRC)

The clinical research industry often evaluates site businesses using visible but incomplete measures: number of sites, number of investigators, therapeutic area (TA) coverage, geography, enrollment history, or claimed patient access. These measures matter, but they can mask the real driver of performance: operating model.
A freestanding research clinic, an embedded private-practice site, a hospital-based research department, a network-affiliated independent site, and a site using employee versus contracted principal investigators (PIs) and/or coordinators may all be called “sites.” They may share the same label, but they differ greatly in how they are built, managed, governed, and held accountable.
Site businesses also differ by whether they are wholly owned and fully integrated, wholly owned but only partially integrated, or affiliated without true ownership. These distinctions materially affect brand architecture, control, patient access, investigator engagement, quality oversight, start-up speed, economics, scalability, and enterprise value.
The path used to expand the platform matters. De novo expansion is generally the cleanest way to achieve full integration because each new location can be built from the same brand architecture, accounting processes, HR systems, CTMS, SOPs, quality framework, training model, and management cadence from day one. Acquisitive growth can add footprint, but it often imports legacy systems, local brands, inherited workflows, and cultural variation that must later be integrated. This distinction is important because the industry is under pressure to execute trials faster, more consistently, and closer to patients.
For many commercial outpatient Phase 2-4 trials, the strongest operating architecture is a centrally governed hybrid model combining freestanding research clinics with embedded private-practice research operations and a disciplined investigator model. Freestanding clinics provide operational discipline, controlled workflows, research-native infrastructure, and speed. Embedded private-practice research operations and contracted private-practice PIs provide patient access, physician trust, therapeutic-area relevance, and community-based recruitment. Employee PIs and employee sub-investigators (sub-Is) can strengthen availability, continuity, and operating control.
This model is materially different from a traditional site network or historical site management organization (SMO) model. Site networks may aggregate independently owned sites and provide services, but aggregation is not the same as control. A network can create breadth without ensuring consistent execution. It can provide services without owning the local operating environment. It can increase nominal footprint while leaving sponsors, CROs, investors, and boards exposed to site-level variability.
This three-part series, which covers operating model pros, cons, and recommendations, is written from an operator’s perspective. The author leads Paradigm Clinical Research, a governed hybrid platform, and believes the model’s advantages are demonstrable in Paradigm’s own operating performance. That perspective should be understood as informed advocacy rather than neutral analysis.
Why Site Operating Model Matters
“Site” is one of the most imprecise words in clinical research. A site can mean a dedicated freestanding research clinic, a physician practice with embedded research operations, a hospital department, an academic medical center (AMC), an independently owned research business affiliated with a network, a physician office receiving central services from an SMO-style organization, a wholly owned location operating under a common integrated platform, a wholly owned location still operating under a legacy or local brand, a loose referral arrangement, or a hybrid platform combining several of the above.
These models may look similar in a feasibility questionnaire. They may all report therapeutic experience, investigator names, patient databases, and enrollment history. But they are not the same. The crucial difference is operating model: how the site is built, governed, staffed, and made accountable for execution. Operating model determines who controls the staff, SOPs, quality, recruitment, start-up, sponsor/CRO communication, escalation, and actual patient-access pathway.
The industry has historically overemphasized reach and underweighted control. For sponsors and CROs, the practical pain point is variability: sites that start slowly, under-enroll, communicate inconsistently, or produce uneven data quality do not merely create inconvenience ― they affect enrollment timelines, data reliability, and ultimately the conduct and risk profile of the study. Those risks are not random. They are often symptoms of operating model and governance. Sponsors and CROs increasingly need sites that can start quickly, enroll predictably, execute consistently, and communicate clearly. Investors and boards increasingly need to understand whether a site business is a true operating platform or merely a collection of relationships.

A Taxonomy Of Clinical Research Site Operating Models
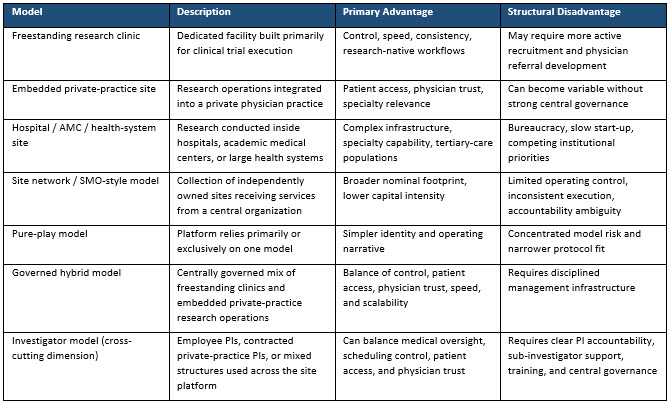
The commercial clinical research site market includes several materially different operating models. The taxonomy below distinguishes the core models by their control profile, primary advantage, and structural disadvantage. Ownership, integration, growth path, and investigator model are separate but related dimensions also addressed below.
Before moving into a more detailed critique of the major operating models, it is worth pausing on a common claim in the site organization market: 'wholly owned sites.' Ownership can be meaningful, but it does not, by itself, prove that a site organization operates as one integrated platform.
Ownership Is Not the Same as Integration
The operating model discussion needs to distinguish legal ownership from operational integration. A site business can wholly own multiple locations and still operate like a loose collection of acquired local businesses if those locations retain separate brands, inconsistent SOPs, different technology, local management norms, variable quality practices, or divergent sponsor/CRO communication patterns.
A fully integrated, wholly owned platform is different. It operates under a common brand, common operating system, common quality framework, common technology stack, centralized training, aligned performance metrics, and clear management authority. In that model, ownership and integration reinforce each other.
Brand architecture matters because it is one of the most visible indicators of integration. A single consistent brand does not, by itself, prove operational integration. But the absence of one consistent brand is a warning signal. It suggests that the company may be legally consolidated without being fully operationally integrated. For sponsors, CROs, investors, and boards, that distinction should be part of diligence.
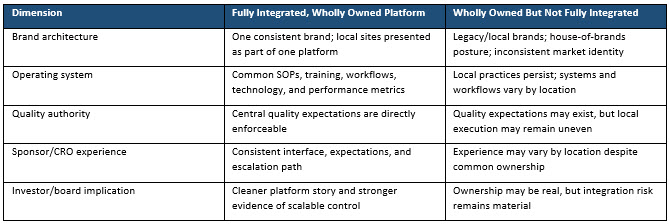
Table 2. Diligence Considerations for Sponsors and CROs: Wholly Owned Does Not Always Mean Fully Integrated.
Ownership and integration are separate dimensions. Legal ownership alone does not prove that a site business operates as one integrated platform, and sponsors and CROs should consider the indicators below when assessing whether a site organization is truly integrated.
The most important distinction is simple: A governed hybrid model is not a site network, and legal ownership is not the same as operational integration.
Integration And Growth Path: De Novo Versus Acquisitive Expansion
Integration is affected not only by ownership structure but also by how the footprint was built. De novo expansion is usually the easiest path to true integration because the organization designs each location from the beginning as part of one platform. The site can launch under the same brand, use the same accounting system, follow the same HR practices, operate in the same CTMS, apply the same SOPs, report through the same management cadence, and adopt the same quality expectations before local habits harden.
Acquisitive growth can be strategically useful when it adds experienced investigators, established patient access, local market credibility, or immediate revenue. But acquisition also imports complexity. The acquiring platform may inherit different brands, compensation structures, accounting practices, HR policies, CTMS configurations, source-documentation habits, regulatory file practices, vendor relationships, and quality norms. Each of those differences creates integration work after the transaction closes.
This is why a company can be wholly owned but still not fully integrated. Legal ownership may change in a single transaction. Operational integration does not. It requires deliberate post-close conversion of systems, workflows, brand identity, personnel expectations, reporting structures, and quality standards. Until that occurs, the business may remain a portfolio of acquired sites rather than a single operating platform.
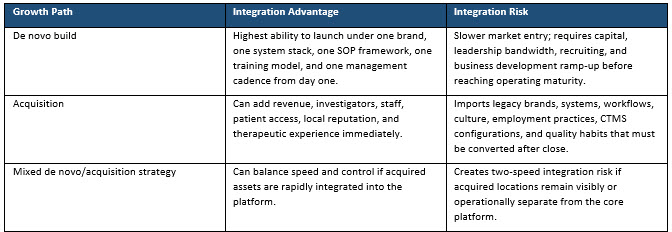
Table 3. Integration implications of de novo versus acquisitive growth.
Part Two: Site Operating Models Performance
In part two, learn how freestanding clinics, embedded private-practice sites, investigator structures, site networks, hospital/academic models, and pure-play approaches perform across access, control, speed, quality, accountability, and scalability. This second article also highlights where each model creates advantage, where it introduces structural risk, and why model fit matters for commercially executable outpatient trials.
About The Author:
 Kurt Mussina is president and a member of the board of directors of Paradigm Clinical Research. With more than 30 years of experience across clinical research, CRO, CDMO, and biopharmaceutical industries, Kurt has built and scaled organizations, driven profitable growth, and fostered long-term relationships with sponsors, CROs, and the broader clinical research community.
Kurt Mussina is president and a member of the board of directors of Paradigm Clinical Research. With more than 30 years of experience across clinical research, CRO, CDMO, and biopharmaceutical industries, Kurt has built and scaled organizations, driven profitable growth, and fostered long-term relationships with sponsors, CROs, and the broader clinical research community.
Prior to Paradigm, Kurt spent a decade with Fresenius Medical Care, where he served as senior vice president and president of Frenova Clinical Research Services. Earlier in his career, Kurt served as president of Triangle Research Labs and as senior vice president of Aptiv Solutions, which was acquired by ICON. His experience also includes executive roles spanning commercial operations, research and development, and business development at Applied Analytical Industries, Inceutica, Inveresk Research, CRF Health, Aptuit, and PharmaCyte Biotech.
Kurt’s early career began as a chemist with Teva Pharmaceuticals and Novartis before earning his MBA from Duke University.