
Why The Governed Hybrid Site Model Is Strategically Superior — Part 3
By Kurt Mussina, CEO, Paradigm Clinical Research, and co-founder, Association of Multisite Research Corporations (AMRC)

In this third and final article of the series of site operating models, the focus shifts from them to defining what a stronger model looks like in practice. Based on my experience, the governed hybrid platform provides a deliberate balance of patient access and physician trust that comes from embedded private-practice relationships, combined with the operational control, speed, quality discipline, and scalability of a centrally managed research organization. Note the model’s performance highlights. But, as with any decision, be sure to weigh your options carefully. Capping off this series are questions and checklists to help guide your site selection activities.
The Governed Hybrid Model
The governed hybrid model combines complementary assets in commercial outpatient research:
- Freestanding research clinics,
- Embedded private-practice research operations, and
- An investigator structure that can balance employee control with private-practice patient access.
Freestanding clinics provide control, speed, research-native workflows, staff accountability, quality consistency, sponsor/CRO responsiveness, and operational scalability. Embedded private-practice sites and contracted private-practice PIs provide patient access, physician trust, specialty relevance, chart-level identification, community reach, referral credibility, and longitudinal care relationships. Employee PIs and employee sub-Is add availability, continuity, and execution support.
The hybrid platform is stronger because it avoids the narrowness of pure-play models. It is not limited to freestanding recruitment infrastructure. It is not dependent solely on physician-practice variability. It is not trapped inside hospital bureaucracy. It is not merely coordinating independent network affiliates. And it is not forced to choose between employed PI control and private-practice PI patient access. The model works because it combines access and control.
This logic is aligned with AMRC’s broader advocacy that multisite clinical research corporations should be understood as strategic infrastructure capable of delivering speed, consistency, reliability, and operational performance.1
The table below shows how a governed hybrid model combines the strengths of freestanding clinics and embedded private-practice research while using governance to reduce the weaknesses of each. The point is not that every protocol requires every component, but that a governed hybrid platform has more ways to match protocol needs without sacrificing operating control.
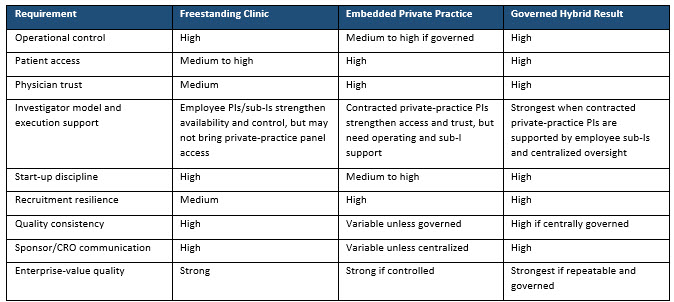
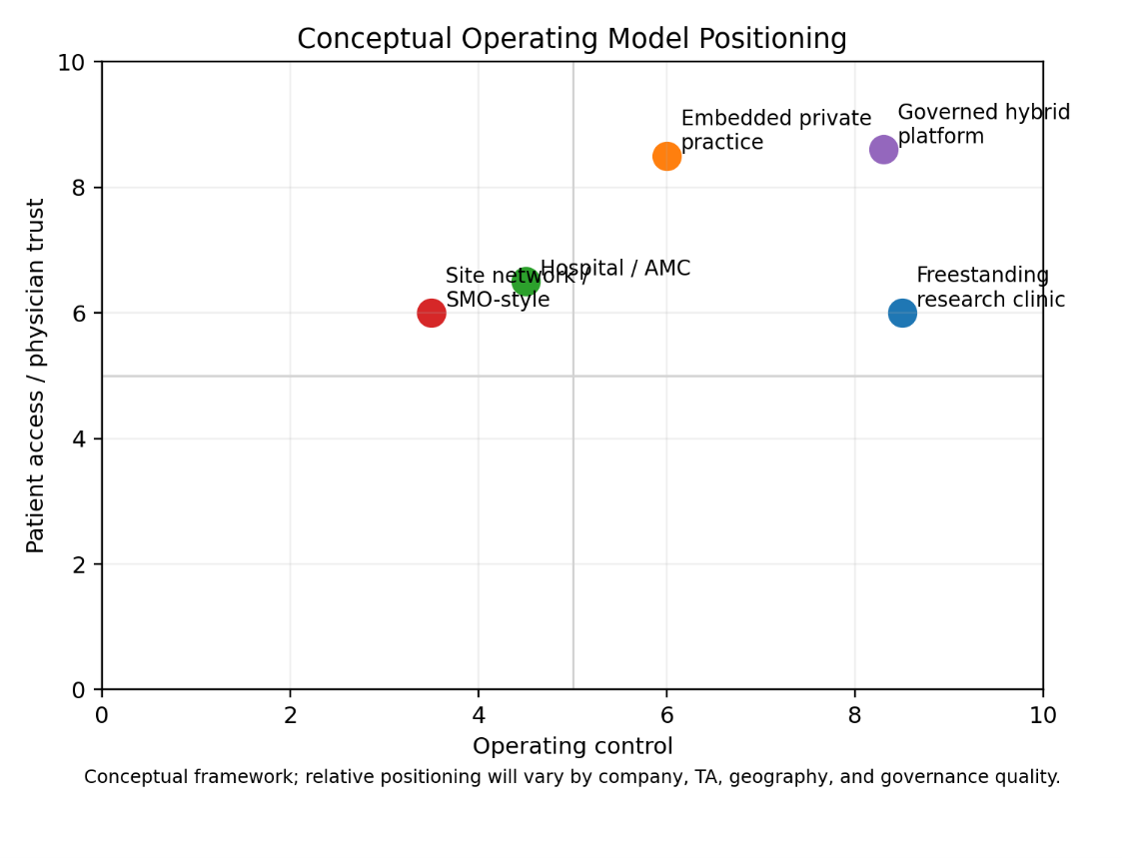
Figure 2: Conceptual operating model positioning. The governed hybrid model is designed to combine the control profile of freestanding research clinics with the patient access and physician trust advantages of embedded private-practice operations. Investigator model is a cross-cutting dimension not shown on these two axes; it affects both operating control and patient access.
Governance: The Difference Between Hybrid Strength and Hybrid Chaos
The hybrid model only works if it is governed. A poorly governed hybrid model can become confusing, inconsistent, and difficult to manage. A well-governed hybrid model creates strategic advantage. The non-negotiable requirement is central operating control.
A serious hybrid platform requires central control across three areas:
Operating infrastructure: common SOPs, centralized training, common CTMS, centralized regulatory oversight, centralized budget and CTA management, and shared performance dashboards.
Quality and accountability: central quality oversight, internal audit or quality assurance (QA) review, corrective-action authority, and defined PI and sub-I expectations with contracted-PI engagement standards.
Sponsor/CRO interface: standardized recruitment workflows, centralized sponsor/CRO communication standards, escalation pathways, and consistent participant experience expectations.
Hybrid does not mean decentralized chaos. It means controlled flexibility. The strategic advantage comes from combining local patient access with central execution discipline. AMRC’s 2026 positioning work is useful here because it directly connects sponsor/CRO priorities to speed, consistency, reliability, and operational performance — the exact outputs a governed hybrid platform is designed to deliver.1
Implications For Stakeholders
If operating model is the next competitive frontier, each stakeholder group should ask a different version of the same core question: Is this a controlled, repeatable operating platform, or a collection of sites, physicians, and relationships that may perform unevenly?
The implications below translate the paper's operating-model argument into practical questions for site operators, physician-research firms, investors and boards, and CROs/sponsors.
For site operators
Clinical research site companies should ask whether they are building a controlled platform or a loose collection of locations. Specifically, they should ask:
- Do we have durable patient-access channels?
- Are physician relationships structured or informal?
- Are PIs employees, contracted local physicians, or a managed mix?
- Do employee sub-Is support physician PIs?
- Do we control the staff who determine execution?
- Are SOPs consistently enforced?
- Is recruitment overly advertising-dependent?
- Is growth adding true operating capacity rather than simply adding site count?
They should also ask whether ownership, branding, systems, investigator model, and day-to-day operations reinforce one platform or reveal fragmentation. Growth is not simply adding sites. Growth is adding controlled, productive, quality-consistent operating capacity.
For physician-research firms
Physician-research firms and private practices entering clinical research should avoid two extremes: treating the physician practice as a passive referral source or expecting the practice to become a fully capable research operation without professional infrastructure. The better model is an embedded operating partnership.
In that partnership, the physician practice and contracted private-practice PI can contribute patient access, clinical credibility, specialty knowledge, investigator judgment, trust-based referral, and longitudinal care relationships. The research platform contributes employee research staff, employee sub-Is where appropriate, SOPs, training, regulatory systems, sponsor/CRO communication, recruitment analytics, budget and CTA support, quality oversight, technology, and performance management.
Patient access is not merely a database issue. It is also a relationship issue. Healthcare providers are highly trusted sources of clinical-trial information and can play an important role in raising awareness and encouraging participation. Embedded private-practice models are structurally positioned to build on that trust and patient relationships, provided the research operation is professionally governed.

For investors and boards
For investors and boards, site operating model is a valuation issue. A business with direct control over staff, systems, quality, recruitment, investigator engagement, PI/sub-I support, and sponsor/CRO communication should be valued differently from a loose network or service-based aggregator. Integration quality is part of that valuation question: a wholly owned business that has not unified its brand, systems, quality structure, investigator model, and performance management may deserve less credit for platform control than a fully integrated business.
The diligence question should not be, “How many sites are there?” The better question is: how much of the operating capacity is controlled, repeatable, quality-consistent, and economically durable? That is the valuation question.
For CROs and sponsors
CROs and sponsors should evaluate sites based on protocol-model fit. The best site partner is not always the largest, most institutional, or most geographically broad. The best partner is the one whose operating model matches the study’s actual needs.
CROs and sponsors should ask:
- Is the site owned, embedded, affiliated, or network-supported?
- Are PIs employed, contracted, or mixed?
- Do contracted private-practice PIs bring active patient access?
- Do employee sub-Is support execution?
- Who employs the research staff?
- Who owns the SOPs?
- Who controls quality oversight?
- Who manages study start-up?
- Who negotiates the budget and CTA?
- Who is accountable for recruitment?
- How are embedded practices governed?
- Are affiliated or network sites clearly distinguished from controlled sites?
- Can the platform enforce corrective action?
They should also ask whether wholly owned sites operate under one brand, one technology stack, one quality system, and one management cadence.
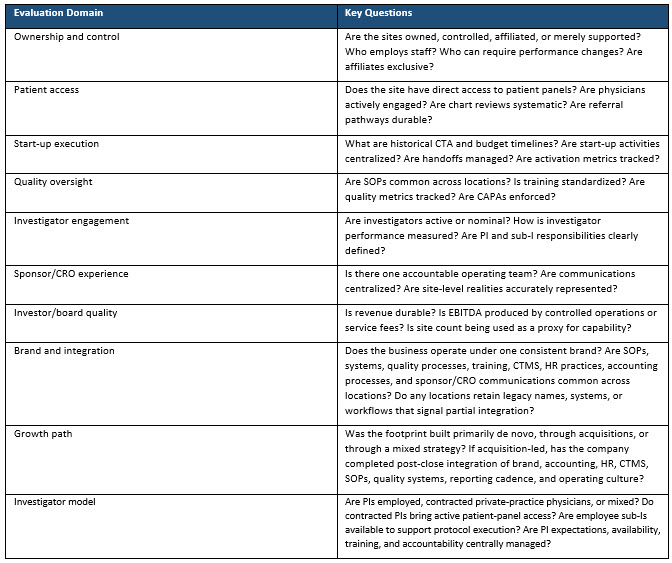
Operating Model Evaluation Checklist
The checklist below is intended as a practical diligence tool for evaluating whether a site organization has true operating-model strength. It can be used by sponsors and CROs during site selection, by investors and boards during platform diligence, and by site operators assessing whether growth is adding controlled capacity or simply adding nominal footprint.
Conclusion
The clinical research site industry is moving beyond the era in which site count, geographic breadth, or therapeutic-area lists were enough to define platform strength. The next competitive frontier is operating model.
Freestanding research clinics provide control, speed, process discipline, and research-native execution. Embedded private-practice sites and contracted private-practice PIs provide patient access, physician trust, specialty relevance, and community-based recruitment. Employee PIs and employee sub-Is provide continuity, availability, and additional execution support. Combined under one disciplined operating system, these elements create a stronger and more resilient model than any single element can provide alone.
Pure-play models each have structural limitations. Freestanding-only platforms may be operationally strong but less connected to treating physician patient panels. Embedded-only platforms may have strong patient access but require rigorous governance to avoid variability. Employee-PI-only models may strengthen control but may not create the same private-practice patient access. Contracted-PI-only models may strengthen access but require sub-I support and central governance to avoid execution risk. Hospital-heavy models are essential for some trials but often mismatched for commercial outpatient research. Site networks and SMO-style models can create breadth, but they may lack the direct operating control necessary to ensure consistent execution.
The strongest commercial site platforms will be those that combine access and control. For sites, that means building operating architecture, not just footprint. For physician-research firms, it means embedding research professionally, not casually. For investors and boards, it means distinguishing true operating platforms from loose aggregations. For CROs and sponsors, it means selecting sites based on protocol-model fit rather than surface-level scale.
The author’s position is intentionally transparent: Paradigm Clinical Research operates as a governed hybrid platform, and this paper reflects the view that the advantages of that model are observable in the way integrated site businesses perform.
Growth path is part of that operating-model assessment. De novo expansion is usually the cleanest route to full integration because it avoids inheriting legacy brands, systems, workflows, and cultures. Acquisitive growth can be valuable, but only if the acquired locations are deliberately converted into the same operating platform rather than left as a portfolio of locally distinct businesses.
Operating model is no longer a back-office detail. It is strategy. It is risk management. It is enterprise value. And it is becoming one of the clearest ways to distinguish durable clinical research site platforms from weaker, less controlled alternatives.
Author’s note: This white paper was authored by Kurt Mussina, CEO of Paradigm Clinical Research and Co-Founder of the Association of Multisite Research Corporations. The paper was developed with drafting and editorial assistance from ChatGPT and Claude. The author directed the framing, reviewed and revised the content, and is responsible for publication judgment and final content.
References:
- Association of Multisite Research Corporations (AMRC). “AMRC publishes 2026 positioning paper.” January 15, 2026. https://amrc.org/news/amrc-publishes-2026-positioning-paper/
About The Author:

Kurt Mussina is CEO of Paradigm Clinical Research. With nearly 40 years of experience across clinical research, CRO, CDMO, and biopharmaceutical industries, Kurt has built and scaled organizations, driven profitable growth, and fostered long-term relationships with sponsors, CROs, and the broader clinical research community.
Prior to Paradigm, Kurt spent nearly a decade with Fresenius Medical Care (FMC), where he built Frenova, FMC’s clinical research site business, and served as the company’s President. He previously served as President of Triangle Research Labs and Senior Vice President of Aptiv Solutions, which was acquired by ICON. His experience also includes executive roles spanning global commercial operations, research and development, and business development at some of the world’s leading contract research services providers.
Kurt began his career as a chemist with Teva Pharmaceuticals and Novartis. He later earned his MBA from Duke University and moved into leadership roles focused on biopharma operations and strategic partnerships.