
Why "Steady Evolution" Best Describes AI's Future

By Dan Schell, Chief Editor, Clinical Leader

When I hosted a recent Clinical Leader webinar on AI in clinical trials, I expected the discussion to focus heavily on technology. Instead, much of the conversation centered on something far less glamorous: the realities of change management in an industry that has historically adopted new technologies far more slowly than outsiders often expect.
The idea for the webinar came from Clinical Leader Editorial Advisory Board member Samir Shah. After he and fellow consultant Brian Whitlock presented on the topic at the TD Cowen Healthcare Conference, Shah suggested the discussion would make a valuable webinar for the Clinical Leader audience. Joining him were veteran clinical development leaders Mark Travers, previously with Merck & Co, and Sheryl Jacobs, formerly of Amgen, who helped ground the discussion in practical experience rather than AI hype.
Collectively, the panel delivered a message that many in the industry may not want to hear: AI will almost certainly change clinical trial operations, but the transformation will be gradual, uneven, and far more dependent on people and processes than on technology alone.
The Industry Has Seen This Movie Before
One of the webinar's recurring themes was that AI is generating tremendous excitement, but clinical development has historically been cautious when adopting new technologies. Shah pointed to previous industry transitions, including EDC, CDISC standards, and DCTs. Each generated significant enthusiasm, yet each took years to achieve meaningful adoption.
“We have to think about our sector and the fact that analogous tech adoption curves have taken quite a bit of time; slow to adopt given stringent regulatory environment quality standards and data safety concerns,” Shah said.
That perspective was echoed by both Jacobs and Travers. “I looked at EDC, I looked at ECOA, I looked at RBQM, and typically pharma is slow to adopt,” Travers said. Jacobs noted that even technologies supported by regulators often require years before sponsors become comfortable implementing them broadly. “I think the industry pulled back a bit from implementation even of RBQM until some of that alignment had a chance to pan out over several years,” she said.
The message was not that AI will fail to gain traction. Rather, history suggests the adoption curve will likely be slower than many current headlines imply.
Separating The Hype From The Reality
The panel also spent considerable time discussing the sheer volume of AI-related noise currently circulating throughout the industry. Shah referenced conference presentations, vendor claims, consulting reports, and the growing number of AI investments being made across life sciences. He noted that nearly every supplier and sponsor discussion now seems to include AI in some form.
That environment has made it increasingly difficult for ClinOps leaders to determine which claims are realistic and which are aspirational. Part of the challenge is that many of the most impressive AI success stories are being presented as isolated use cases. A particular function may achieve a significant efficiency gain, but that does not necessarily translate into equivalent savings across an entire development program.
The panel repeatedly urged attendees to look beyond headlines and focus on operational realities, regulatory requirements, and implementation challenges. In other words, AI may eventually transform clinical development, but getting from a successful proof of concept to enterprise-wide adoption is a very different challenge.
AI Is Already Here, Just Not Where Most People Think
Another important distinction made during the discussion was between AI's current use and its future potential. According to Jacobs, AI has already gained traction in drug discovery and target identification. Clinical development, however, remains more cautious, particularly when AI touches data that will ultimately support regulatory submissions. “In development, there's been a lot slower adoption,” Jacobs said. “Many sponsors and CROs are utilizing AI in areas that are maybe not necessarily impacting the clinical data used in your dossiers (e.g., country and site selection, status tracking, workflow automation, operational support functions). “I think it's probably several years out until we start seeing some of the AI pieces used in actual data for submissions.”
Travers agreed that adoption will likely occur function by function rather than through a single enterprise-wide implementation. “It will not be an end-to-end solution,” he said. “I think there'll be elements of that clinical trial process where AI is showing to be of great value.”
Big Pharma & Small Biotechs Will Use AI Differently
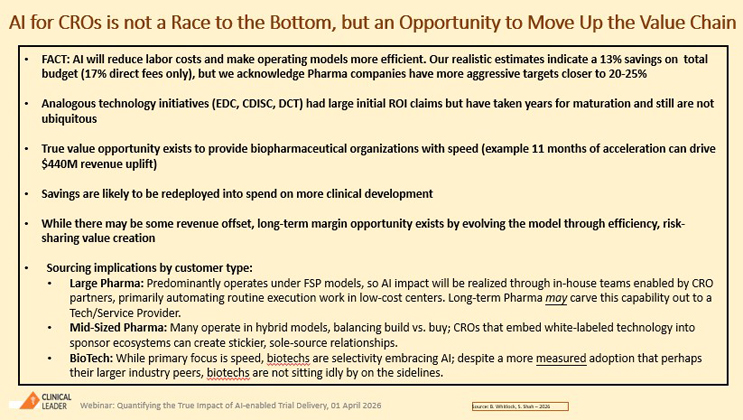
One of the more nuanced discussions during the webinar focused on the fact that AI adoption will likely follow different paths depending on a company's operating model. For example, large pharmaceutical companies and small biotechs are approaching AI from very different starting points. Large sponsors often operate under FSP models and maintain significant internal infrastructure. As a result, many view AI as a capability that should be developed internally and integrated into existing systems.
Of course, that creates new challenges for CROs, which have traditionally developed technology within their own ecosystems. Going forward, sponsors may expect tools that can operate inside sponsor environments rather than requiring companies to adopt entirely new platforms.
Smaller biotech companies face a different reality. Many rely heavily on FSO models and maintain lean internal organizations. For those companies, AI may arrive through CRO partnerships rather than internal development efforts.
At the same time, biotechs often have limited resources and appetite for funding extensive technology development. Jacobs noted that sponsors and CROs will need new conversations regarding who pays for innovation and how emerging technologies are deployed.
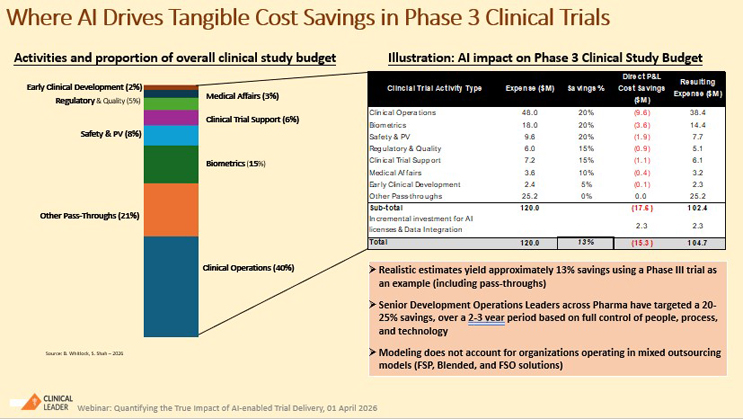
The Cost Savings Debate
Drawing from work originally presented at the TD Cowen conference, Whitlock modeled a hypothetical Phase 3 oncology study and estimated that a fully AI-enabled environment could reduce total trial costs by approximately 13%. While the exercise provided useful context, Whitlock was cautious with this info, saying, “I don’t want anyone running out of this call saying, ‘We're going to save 13% on a trial if we heavily utilize AI!’”
Travers was even more direct. “Please don't show these previous slides to finance directors and VPs,” he joked. “All they will see is cost savings, cost reduction, reduction in headcount.” Instead, he urged organizations to focus first on quality and speed improvements rather than workforce reductions. Jacobs added that every company begins from a different baseline and that savings will vary based on existing processes, maturity, and operational efficiency.
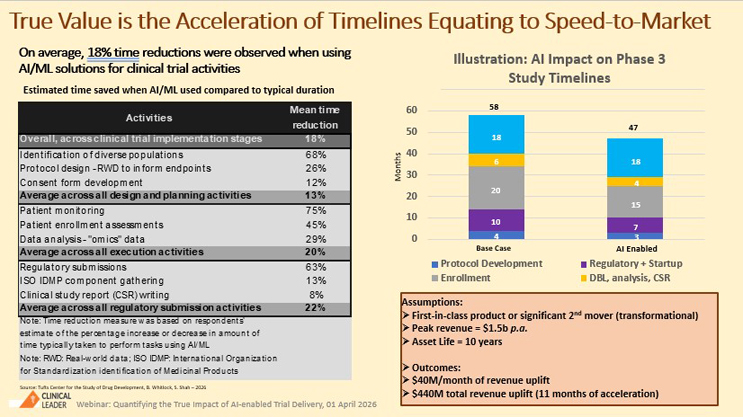
Speed, Value, And The Future Of CROs
If there was one area where the panel seemed especially optimistic, it was AI's potential to shorten clinical trial timelines. Whitlock’s model suggested a hypothetical Phase 3 oncology study could potentially shrink from 58 months to 47 months through broad AI enablement. “You can save $15 million on your trial budget,” Whitlock said. “You can also accelerate your asset into a commercial setting by months and generate tremendous amount of value as an organization as well as for the patients that you're serving.”
The discussion expanded beyond sponsor organizations and into what AI may mean for CROs. For instance, Whitlock argued that projected efficiency gains should not automatically be interpreted as a threat to the service-provider industry. Instead, CROs may need to evolve beyond traditional time-and-materials business models. Rather than simply selling labor, CROs may increasingly compete based on the value they create, the insights they generate, and the outcomes they help sponsors achieve. Shah agreed, noting that improved efficiency may allow sponsors to pursue additional development opportunities rather than simply reducing spending.
The implication was clear: the biggest benefit of AI may not be cost reduction. It may be enabling sponsors to run more studies, test more assets, and bring therapies to patients faster.
No Surprise: Culture May Be The Problem
No proposed change in pharma is going to be free of a change management bottleneck, and AI in clinical trials is surely going to suffer from this. Jacobs cautioned against top-down mandates that fail to involve operational teams responsible for executing clinical trials. “Those initiatives that come only top down tend to fail because they meet resistance of the actual folks who are on the ground doing the day-to-day work,” she said. Those folks on the ground are the ClinOps professionals who understand where inefficiencies exist and where automation can create meaningful value.
The panel also pushed back against narratives that frame AI primarily as a headcount reduction exercise. Both Travers and Jacobs argued that organizations should focus on freeing employees from administrative work and allowing them to spend more time on activities that directly support patients and study execution.
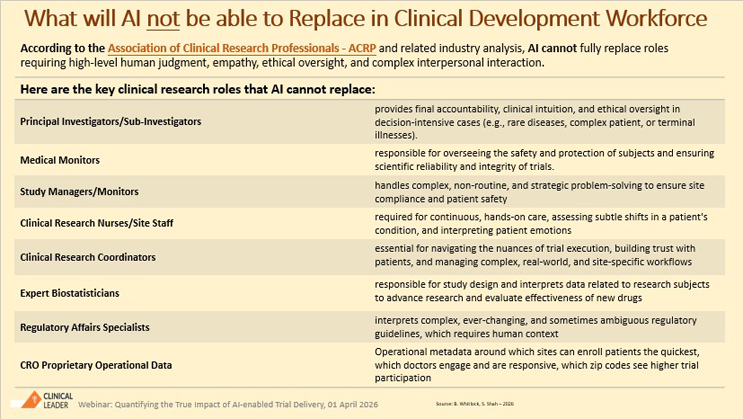
As the conversation turned toward long-term adoption, the panel generally agreed that AI will eventually become a standard expectation rather than a competitive differentiator. Much like offshore delivery, EDC, and risk-based monitoring before it, AI may ultimately become part of the industry's baseline operating model. Shah said, “We don't think that AI is going to replace everything that's in the clinical development workforce.”
That may be the most important takeaway from the discussion. The industry is no longer debating whether AI will influence clinical trial operations. The debate now centers on how quickly adoption will occur, where value will be created, and how organizations can separate realistic opportunities from unrealistic expectations.
Let’s face it; we’ve heard this before. The future of AI in clinical trials is not a story of sudden disruption. It is a story of steady evolution, guided by operational realities, regulatory oversight, and the people responsible for delivering clinical trials every day.